Where are we with Covid-19 today?
In the early 2021 global population, especially in the developed world, received a lot of positive signals about ‘back to normal’ being close. All hopes are with the rapid rollout of vaccination. As of March 21, 458 million doses were administered. This amounted to at least partial coverage of roughly 223 mln people, twice more than those who were infected with SARS-CoV-2 and tested positive (124 mln) [1].
The need to vaccinate to overcome the pandemic has been “sold” by most governments as a foregone conclusion and the only possible way to get economies and societies in general back on track long before any vaccine was developed. The public debate is not focused on strengthening citizens’ immune systems to mitigate a disease flow, taking simple precautionary measures, providing information on COVID-19 treatments’ research (medicines that a person with symptoms can take as a cure) in parallel to vaccines and testing people for antibodies to prevent unnecessary or delay scheduled vaccination in case a person’s body has already been exposed to a virus and set off coping mechanisms on its own. Regarding the latter claim, according to a study published in the “Science” journal, COVID-19 leads to generation of substantial immune memory (around 95% of people retained immune memory at ~6 months after infection).
Instead public discourse is centered around the types and brands of vaccines, vaccination schedule and jabs’ availability. In other words, the question is “which one and when” and not “why at all”. While many people are cautious about vaccination, governments try hard to persuade them to take a jab. Their argument is simple – ‘just do it’ for your own and public good. However, we believe that pharma and governments in a meantime are paying themselves very poor service by failing to provide for proper liability mechanisms tied to vaccination. This issue must be properly addressed and not overlooked, bypassed or skipped*. Only then will vaccination hesitancy rates truly go down. Until the moment people are reassured, news akin to halting AstraZeneca vaccination rollout in a number of countries due to emerging concerns are only going to deepen public distrust and willingness to avoid a risk.
* Update 1 from 26 April 2021: This statement concerns rather countries of the EU. For 92 low and middle-income countries that get the vaccines in the frame of WHO’s covax system, the compensation will be foreseen without the resort to the law courts – https://www.who.int/news/item/22-02-2021-no-fault-compensation-programme-for-covid-19-vaccines-is-a-world-first; in Ukraine, the compensation has been foreseen with the Decree of the Cabinet of Ministers from 31 March 2021
The way people are both encouraged and shamed/coerced to taking a vaccine is a separate subject. Here it is mentioned briefly to expose that “vaccination rush” carries not only positives with alleged comebacks to normality, but also numerous negatives, some of which we will consider below.
When benefits outweigh the risks
As a rule of thumb, vaccination is (strongly) recommended when it is scientifically proven through a long and meticulous process that the benefit to vaccination far outweighs risks related to possible side effects and long-term complications caused by a vaccine.
In case of existing COVID-19 unapproved vaccines [2]:
- none has been given a definitive unconditional authorisation as simply not enough time has passed to observe any potential adverse reactions over time (in the US the “vaccines” have got an “Emergency use authorization”, by the WHO – “Emergency use listing”, and in the EU – “Conditional marketing authorisation”);
- some of marketed products commonly referred to as vaccines belong to a category of mRNA type of vaccines which is a scientific novelty and has never been used for inoculation before, let alone a mass one;
- not enough studies have been conducted on compatibility of COVID-19 vaccines with other types of vaccines (i.e. against influenza which is typically also administered among the biggest COVID-19 risk group – elderly);
- not enough studies have been conducted on potential impacts of COVID-19 vaccines on people with underlying medical conditions (such as diabetes, lung disease, cancer, immunodeficiency, heart disease, hypertension, asthma, kidney disease, GI/liver disease, and obesity)
“No liability” clause in purchasing contracts lobbied by pharmaceutical companies
Pharmaceutical companies are taking advantage of governments’ panic and competitive strategies aimed at ensuring that high vaccination rates are achieved in a quickest possible manner. The only stumbling block is that some people (dismissively referred or equating to as “antivaxxers” [3]) question this “vaccine is the only solution” narrative because they do not trust either their own governments or “big pharma”. The distrust comes, among other aspects, from no liability for irreversible adverse events from the vaccines enshrined into purchasing contracts [4] (Figure 1). So how come this fear is not addressed? Why are there no steps foreseen and properly communicated internationally or nationally to provide for mechanisms of responsibility in case of adverse events?
Figure 1. An example of the ‘no liability clause’ from AstraZeneca constract with the European Commission
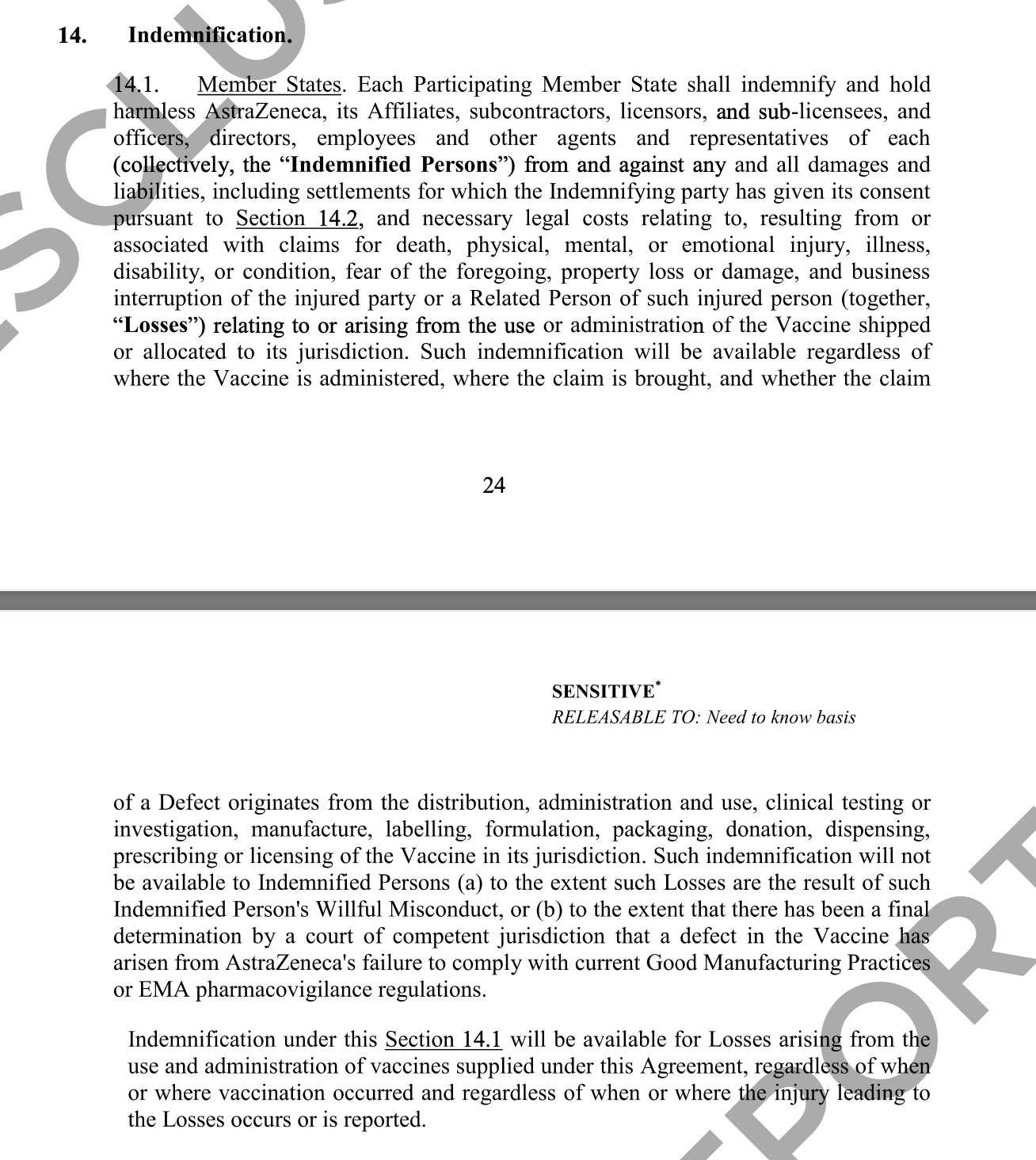
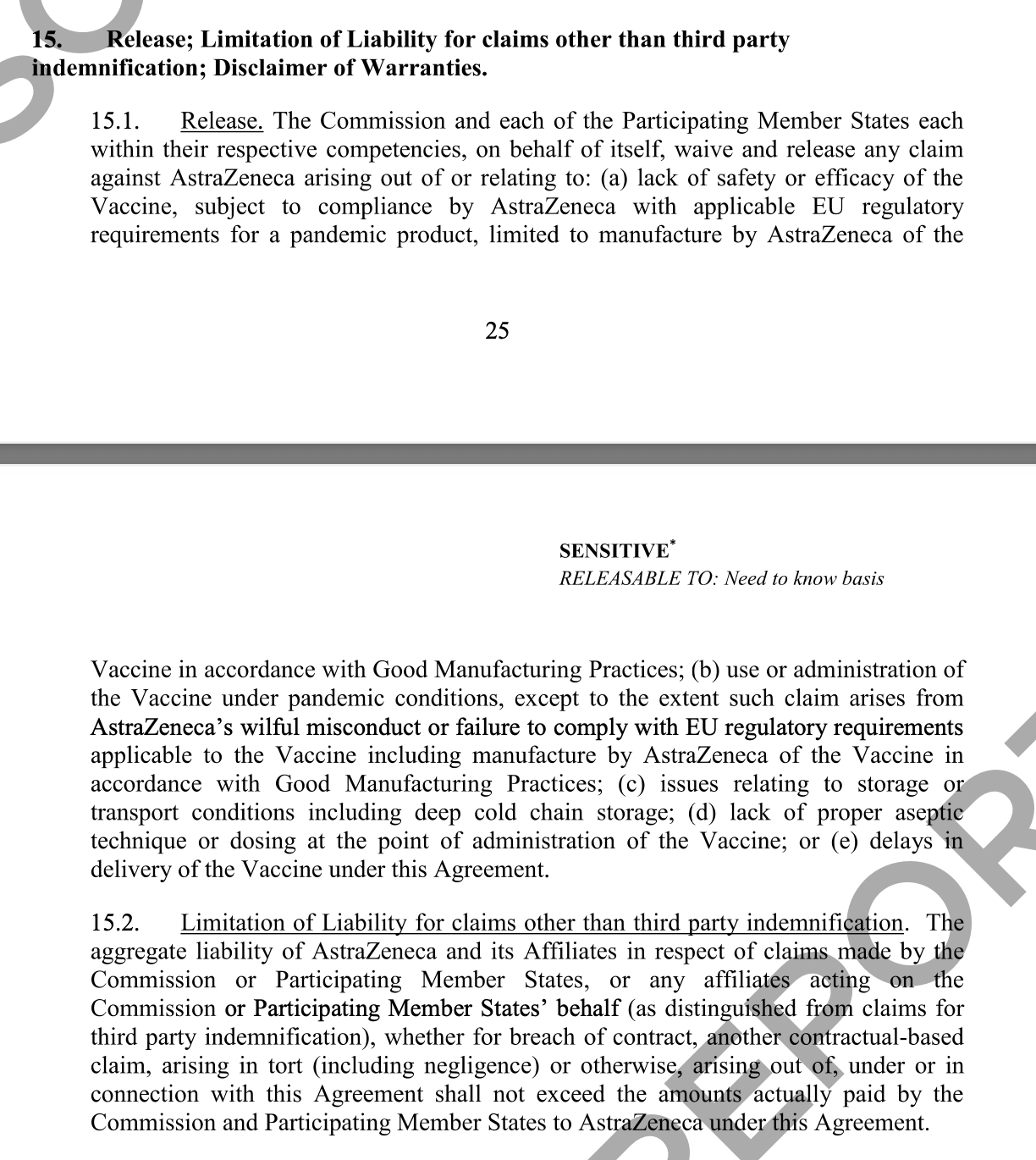
Source: Art. 14, Art. 15 of the Contract of the EU with Astrazeneca
Most governments claim that the COVID-19 vaccine is not compulsory, but at the same time, they increasingly enable social and political pressure on their citizens, often by referring to the notion of “solidarity”. They claim that the vaccines are efficient and safe but, at the same time, they do not hurry to prove their convictions by putting in place the mechanisms of liability**. But would not the latter show the confidence of a state in THE solution and help win more “hearts and minds” of people? Apparently not, because while we are to believe the numbers provided by vaccines’ manufacturers about their effectiveness, there is no reliable data available regarding their long-term safety (as this can be proven only over time).
** Update 2 from 26 April 2021: his statement concerns rather countries of the EU. The WHO’s covax liability program is not considered.
According to the contracts with the authorities, the COVID-19 vaccine manufacturers are exempt from liability. This exemption has been a necessary precondition for pharmaceutical companies to commence mass production as per advice by private experts and virologists consulting the governments. We also observe that the stimuli to vaccinate arise from these tight circles as well. That is again a different story which we will leave aside. Instead we will consider a logical question: doesn’t the one who exerts pressure and/or the one who “guarantees” safety, have to take responsibility should something go wrong? That is what a guarantee is all about, isn’t it?
In the EU, the Article 7 (e) of the Product Liability Directive 1985 provides that ‘the producer shall not be liable as a result of this directive if he proves that “the state of scientific and technical knowledge at the time when he put the product into circulation was not such as to enable the existence of the defect to be discovered”. In the case of the COVID-19 vaccines, this is the case. The vaccines started being manufactured and administered when the state of scientific and technical knowledge was not such as to enable the existence of the defect to be discovered.
“The Directive 2001/83/EC (the ‘Medicines Code’) contains rules that shield marketing authorisation holders, manufacturers and health professionals from civil liability arising from the use of an unauthorised medicinal product, or from the use of a product otherwise than in accordance with its authorisation, when such use is by the licensing authority in response to (among other things) the spread of pathogens. The public policy rationale behind this principle is to provide a legal protection against exposure to litigation for companies who are willing to innovate into the development and manufacture of vaccinations to tackle global health threats such as COVID-19. The principle established under Article 5(3) of the Medicines Code was implemented into UK law by Regulation 345 of the HMRs. However, the exemption does not extend to the risks posed by defective products. In a UK context, a manufacturer would still hold liability for a defective product that meets the conditions under section 2 of the Consumer Protection Act 1987”.
EU/EMA authorisation despite missing information
Nonetheless, Pfizer, Moderna, AstraZeneca, and Janssen have been given conditional marketing authorization by European Medicines Agency (EMA). Once a CMA has been granted, companies must provide further data from ongoing or new studies within pre-defined deadlines to confirm that the benefits continue to outweigh the risks.
Thus, Pfizer will submit a final report on the study, the third phase of which is currently still ongoing, until 31 December 2023, Janssen – until 31 December 2023, AstraZeneca – until 31 March 2024, and Moderna – until 30 June 2024. Only then will EMA approve them definitively, or will not approve, if there are serious side effects, adverse events and/or irreparable consequences. Yet who will be interested in 2024 whether the EMA approves them or not, if by that time hundreds of millions of people in Europe and at least a few billion worldwide will already be vaccinated?
Paragraph 2.7 of the ЕМА Assessment Report on Pfizer vaccine of 21 December 2021 “Risk management Plan. Safety specification” indicates the missing information which will be provided by the manufacturer by the deadlines set in the Report (from 2021 till 2024):
-
- Since pregnant and breast-feeding women were excluded from the study, no information is available for those populations.
- Long-term safety is included as missing information.
- Interaction with other vaccines has not been evaluated in clinical trials and may be of interest to prescribers. As elderly individuals will be one target group for vaccination, and they often may need vaccination with other vaccines such as influenza and pneumococcus vaccines, further data is requested.
- Data from use in frail patients with comorbidities (e.g. chronic obstructive pulmonary disease (COPD), diabetes, chronic neurological disease, cardiovascular disorders), is limited. Therefore, use in frail patients with comorbidities (e.g. chronic obstructive pulmonary disease (COPD), diabetes, chronic neurological disease, cardiovascular disorders) has been included as missing information in the RMP.
- Furthermore, information is limited on the use in patients with autoimmune or inflammatory disorders, as well as in immunocompromised patients. Thus, these groups are also included as missing information. Such missing information will be collected in the post-authorisation safety studies.
This kind of missing information is a part of the EMA Assessment report for every COVID-19 vaccine.
Nothing learnt from pandemix cases?
In 2019 the now prominent Belgian virologist Marc van Ranst was recorded on camera giving a lecture at the Chatham House on “how to sell a pandemic”. He was sharing his communication experience during the swine flu in 2009, the goal of which was to convince the population to vaccinate. In early 2021 the video has been shared thousands of times on social media, prompting a controversial reaction among Belgians. Zooming in on the outcome of the swine flu pandemic and a vaccine as a solution that “had to be sold”, we will find out the following: around 1500 people, including 800 children in Europe developed narcolepsy (sleep disorder) after receiving the swine flu vaccine, Pandemrix. Pandemrix was initially authorised under “exceptional circumstances” due to the urgent need to address the threat of a swine flu pandemic and was administered to 31 million people Europe-wide. The review of Pandemrix after the occurrence of cases of narcolepsy was initiated at the request of the European Commission under Article 20 of Regulation (EC) No 726/2004, on 27 August 2010, following an increased number of reports on narcolepsy in Finland and Sweden. Its marketing authorisation was withdrawn only after 6 years (!) – in 2015. Some people who managed to prove the detrimental effects related to vaccination got compensation under national vaccine injury compensation schemes. In the UK, for example, under the Vaccine Damage Payment scheme the compensation amounted to 120 000 pounds per person.
Trackrecord of pharmaceutical companies
Yet, the tiresome process of claiming compensation rights is a doubtful remedy (even if it was readily available in all countries that embark on vaccination programmes), especially when consequences for one’s life are detrimental or even worse – fatal. The gloom kicks in even deeper when a track record of leading pharmaceutical producers is considered.
In 2009 the American pharmaceutical giant Pfizer Inc. and its subsidiary Pharmacia & Upjohn Company Inc. (hereinafter together “Pfizer”) agreed to pay $2.3 billion, the largest health care fraud settlement in the history of the US Department of Justice, to resolve criminal and civil liability arising from the illegal promotion of certain pharmaceutical products.
Pharmacia & Upjohn Company has agreed to plead guilty to a felony violation of the Food, Drug and Cosmetic Act for misbranding Bextra with the intent to defraud or mislead. Bextra is an anti-inflammatory drug that Pfizer pulled from the market in 2005. Under the provisions of the Food, Drug and Cosmetic Act, a company must specify the intended uses of a product. Nevertheless, Pfizer promoted the product for several so-called “off-label” (not specified) uses and in dosages that authorities specifically declined to approve due to safety concerns.
EU law requires vaccine companies, national authorities and the EMA to follow a number of monitoring (pharmacovigilance) processes after a product has been authorised. The European Centre for Disease Prevention and Control (ECDC) and the European Medicines Agency (EMA), together with the Commission, Member States, European and international partners are conducting effectiveness and safety studies specifically for COVID-19 vaccines. This additional data can also be used to complement regulatory actions as necessary, e.g. changes in the conditions of use, warnings and related changes to product information for health care professionals and patients.
Under the CMA process, vaccine companies are responsible for the continued monitoring of safety of vaccines; reporting of serious adverse events; keeping the product information up to date, conducting safety and effectiveness studies; looking at performance of their products in the larger populations on the market and submitting regular safety and benefit risk reports to the EMA.
But, in the EU, there is no specification on what “vaccine companies are responsible for safety of the vaccine” means for a concrete person that has got a jab and suffered adverse side effects. It is not yet clear who will be responsible for the damage. It is not clear how easy it is to prove the damage: when there is health failure it is not always clear whether it is connected to the jab unless many similar cases are discovered and properly reported, and in the case of death there are often refusals from the side of the authorities to authorise autopsies. There is no proper communication in the EU on the mechanisms of investigation and compensation which makes it more difficult to promote such an important campaign as vaccination.
Compensation mechanisms
Today, the Vaccine Damage Payment in the UK mentioned above is extended to those who may suffer from the damages due to COVID-19 vaccines.
In the USA, a little-known governmental Countermeasures Injury Compensation Program (CICP) provides benefits to people who can prove they suffered serious injury from a vaccine. If a case for compensation through the CICP is successful, the program provides up to $50,000 per year in unreimbursed lost wages and out-of-pocket medical expenses. It won’t cover legal fees or anything to compensate for pain and suffering. It is also capped at the death benefit of $370,376. By now CICP has rejected a majority of the compensation requests made since the program began 10 years ago. Of the 499 claims filed, the CICP has compensated only 29 claims, totaling more than $6 million.
US based lawyers claim that it would make more sense for COVID-19 vaccine injuries to be covered by another programme under the the National Vaccine Injury Compensation Program (NVICP), which handles claims for 16 routine vaccines. The program paid on about 70% of petitions adjudicated by the court from 2006 to 2018. And since it began considering claims in 1988, the NVICP has paid approximately $4.4 billion in total compensation. The COVID-19 vaccines, however, are not on the list of eligible vaccines [5].
The question of compensation mechanisms, therefore, even in the US hangs up in the air, let alone lower-income countries and regions of the world.
In South Korea, there is a mechanism of compensation: a benefit of up to 430 million won (US$388,000) will be provided if someone is severely disabled or dies as a result of taking a COVID-19 vaccine. The government will cover costs for hospital stays and other kinds of treatment costs.
By providing a no-fault lump-sum compensation in full and final settlement of any claims, the COVAX programme aims to significantly reduce the need for recourse to the law courts, a potentially lengthy and costly process.
Issues of liability raised by people’s representatives
Within European structures, the issue of liability was raised, among other concerns, by the European Parliament in September 2020 in the discussion with the representatives of the pharma industry and the European Medicines Agency as well as by Parliamentary Assembly of the Council of Europe in January 2021 in the Resolution “Covid-19 vaccines: ethical, legal and practical considerations”.
The current tendency is for the questions of liability to be raised by the representatives of the people. Yet with little to no replication on either the governmental level, or in the media. However, answering this question in no ambiguous terms is crucial to gaining trust of people who doubt whether to vaccinate or not.
Strangely enough, there are no voices that would push for equal burden sharing among all parties involved: the manufacturer, the government, the medical agency that approves the vaccine, the entity that pressures or forces to vaccinate (such as an employer who puts its employees at risk of losing jobs or even airlines declining boarding without “vaccination certificate”), and a person himself/herself.
In order to be efficient, such an insurance should provide for a mechanism and procedure to prove the connection between the vaccination and an injury, knowing that in the countries with the existing compensation mechanisms the burden of proof is still on the injured person, and often the injuries are not investigated or compensations are declined (or in case of death autopsies are often rejected). At the same time, the amount of compensation in the countries that provide for mechanisms of compensation reveal that most of such claims are legit and legitimate. What is more, they would be legitimate even there where the mechanism is not in place, and therefore justice cannot be served. So why do people who will get vaccinated “out of solidarity/pressure” should stay one-on-one with whatever consequences stemming from “vaccination rush” especially when benefits of COVID-19 vaccination are not (yet) proven to outweigh the risks?
Today, the studies on whether any given “want-to-be-vaccine” prevents one from getting COVID-19 or from infecting others are still ongoing. It is expected though that thanks to a jab (or two) the disease may not be as severe as it would be without it, and that it may prevent death of a person who contracted the virus. In this situation, the “call to solidarity” does not make sense, and if there is no responsibility for the vaccine injury, it should be left to a person to decide whether to vaccinate or not.
Notes
[1] Throughout the text the reference to “infected and tested positive” will be made as a statistically verified data, although it is acknowledged that (1) not everyone who was infected was tested and (2) actual figures are not fully accurate due to false negative and false positive results
[2] See more information on vaccines from FDA (1, 2), and European medicines agency (1, 2, 3), read the difference between FDA approval and authorization here.
[3] See more information on vaccines from FDA (1, 2), and European medicines agency (1, 2, 3), read the difference between FDA approval and authorization here.
[4] Art. 14, Art. 15 of the Contract of the EU with Astrazeneca – p. 24-25. See also p. 1.23.1 of the Advance Purchase Agreement between EC and Curevac- https://ec.europa.eu/info/sites/info/files/curevac_-_redacted_advance_purchase_agreement_0.pdf, see also https://www.statnews.com/2021/02/23/pfizer-plays-hardball-in-covid19-vaccine-negotiations-in-latin-america/ and http://w1.c1.rada.gov.ua/pls/zweb2/webproc4_1?pf3511=71406


Attention
The authors do not work for, consult to, own shares in or receive funding from any company or organization that would benefit from this article, and have no relevant affiliations
